Cost-Utility Analysis of Human Papillomavirus Vaccination and Cervical Screening on Cervical Cancer Patient in Indonesia
Didik Setiawan, MSc, Apt1,2,*, Franklin Christiaan Dolk, MSc1, Auliya A. Suwantika, PhD1,3, Tjalke Arend Westra, PhD1, Jan C. WIlschut, PhD4, Maarten Jacobus Postma, PhD1
1Unit of PharmacoEpidemiology & PharmacoEconomics (PE2), Department of Pharmacy, University of Groningen, Groningen, TheNetherlands; 2Faculty of Pharmacy, University of Muhammadiyah Purwokerto, Purwokerto, Indonesia; 3Faculty of Pharmacy, University of Padjadjaran, Bandung, Indonesia; 4Department of Medical Microbiology, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands; 5Institute of Science in Healthy Aging & healthcaRE (SHARE), University Medical Center Groningen (UMCG), Groningen, The Netherlands
ABSTRACT
Background: Although cervical cancer is a preventable disease, the clinical and economic burdens of cervical cancer are still substantial issues in Indonesia.
Objectives: The main purpose of this study was to model the costs, clinical benefits, and cost-utility of both visual inspection with acetic acid (VIA) screening alone and human papillomavirus (HPV) vaccination in addition to VIA screening in Indonesia.
Methods: We developed a population-based Markov model, consisting of three health states (susceptible, cervical cancer, and death), to assess future costs, health effects, and the cost-utility of cervical cancer prevention strategies in Indonesia. We followed a cohort of 100,000 females 12 to 100 years old and compared VIA screening alone with the addition of HPV vaccination on top of the screening to “no intervention.”
Results: The implementation of VIA screening alone and in combination with HPV vaccination would reduce the cervical cancer incidence by 7.9% and 58.5%, corresponding to 25 and 98 deaths avoided within the cohort of 100,000, respectively. We also estimated that HPV vaccination combined with VIA screening apparently yielded a lower incremental cost-effectiveness ratio at international dollar 1863/quality-adjusted life-year (QALY), compared with VIA screening alone (I$3126/QALY). Both strategies could how- ever be definitely labeled as very cost-effective interventions, based on a threshold suggested by the World Health Organization. The incremental cost-effectiveness ratio was sensitive to the discount rate, cervical cancer treatment costs, and quality of life as part of the QALY. Conclusions: The addition of HPV vaccination on top of VIA screening could be a cost-effective strategy in Indonesia even if relatively conservative assumptions are applied. This population- based model can be considered as an essential tool to inform decision makers on designing optimal strategies for cervical cancer prevention in Indonesia.
Keywords: Cervical cancer, cost-utility analysis, human papillomavirus, Indonesia, vaccination.
Introduction
Cervical cancer is the second most common cancer among women in Indonesia. The age-standardized cervical cancer incidence rate and mortality rate per 100,000 women in 2012 was 17.3 and 8.1, respectively [1]. The long onset of cervical cancer development [2,3] enables the application of cervical screening to prevent and control cervical cancer. Despite the poor sensitivity of visual inspection with acetic acid (VIA) screening [4],it is the most commonly recommended screening strategy for countries with limited resources [5]. Well-organized VIA screening programs definitely decrease the burden of cervical cancer at relatively low costs [6,7]. The Ministry of Health, Republic of Indonesia launched a cervical cancer control program in 2007 and started a campaign recommending VIA screening for all susceptible women [8–10]. Yet, several studies reported various barriers to the implementation of this program, such as limited screening coverage, poor quality of services, and subsequent poor cryotherapy performance [11].\
In addition to the screening program, the introduction of prophylactic human papillomavirus (HPV) vaccination of girls against two high-risk HPV types (16 and 18) [12], which together are responsible for the large majority of cervical cancer development cases, offers primary prevention of cervical cancer [5,7]. There are two available HPV vaccines in the market, and their efficacies against HPV infections and cervical intraepithelial neoplasm have been demonstrated in numerous clinical trials [13–17]. Next to the efficacy and safety of vaccines, the available national budget for vaccination and affordability presents the other main consideration for a country to implement a vaccination program. Although the cost-effectiveness of HPV vaccination has been proven in many studies [18–22], those findings not necessarily apply to Indonesia because many differences in clinical profiles, patient and population characteristics, and health care systems among countries exist.
Although a new health insurance system has been implemented from 2014 onward in Indonesia, pharmacoeconomic studies have not yet been incorporated as a criterion into the decision-making process. However, cost-utility studies on cervical cancer prevention can provide valuable information for the decision maker to design the most cost-effective strategy to reduce the clinical and economic burdens of HPV-related disease among Indonesian women, within the limited budget. The main purpose of this study was to model the costs, clinical benefits, and cost-utility of both VIA screening alone and HPV vaccination in addition to VIA screening in Indonesia. To interpret the findings from this study, we applied the World Health Organization’s (WHO’s) threshold on cost-effectiveness of immunization programs [23,24].
Methods
Model Overview
We developed a population-based Markov model for Indonesia by using Microsofts Excel (Microsoft, Redmond, WA). The model (as shown in Fig. 1) consists of three health states (susceptible, cervical cancer, and death), which represent the major stages throughout the natural history of infection and cervical cancer. In our model, “susceptible for cancer” refers not only to healthy women but also to infected women with cervical intraepithelial neoplasm but (yet) without cancer. This simplification was made to accommodate with the limited data availability in Indonesia; notably, more complicated models would lack the data to populate them. In addition, in annual cycles, women may move through “cervical cancer” and “death” states. We hypothesized a cohort of 100,000 12-year-old girls before sexual debut as the initial situation in the model [25], followed until 100 years old. To estimate the natural history of cervical cancer, we applied the 2012 WHO’s life table on age-dependent incidence and mortality rate specific for cervical cancer in Indonesia [26,27]. The transition from cervical cancer to death resulted from death caused by cancer as well as by other diseases. We performed our analysis from the payer’s perspective, based on national tariffs that were recently launched by the Ministry of Health for all treatments in primary care and hospitals [28].
We compared three strategies in the base case: 1) without any intervention (reference), 2) with VIA screening, and 3) with VIA screening and HPV vaccination. Both unvaccinated and vaccinated groups were followed in the model with differing risks until the potential screening process. Cryotherapy treatment was assumed to be given among a part of positive individuals when precancer stages would be detected. Specific proportions of deaths, cancer cases, and recovered patients followed from VIA screening efficacies related to the prevention of cervical cancer [29]. In addition, we assumed that 15.8% of new patients with cervical cancer will have a recurrence and undergo an additional/ recurrence treatment [30]. The model parameters and baseline values specifically adopted for Indonesia are presented in Table 1.
 |
| Fig. 1 – Markov model for the development of cervical cancer. |
Screening and Vaccination
Despite the extensive communication and the introduction of the national VIA screening program in 2007, the performance of this program remains sub optimal [11]. In our study, we assumed implementation of the screening for 30- to 60-year-old women within an annual interval of 3 years if the previous test result was negative, according to the recommendation [8,9]. We assumed that 63.6% of eligible (“susceptible” in the model) women would undergo VIA screening every 3 years [29]. We applied a detection rate of VIA screening of 69.4% [31] and an adherence rate to cryotherapy of 83.1% [11], based on previous studies in Indonesia. Furthermore, a study by Sankaranarayanan et al. found that the incidence ratio and the mortality hazard ratio for screened women was 0.75 and 0.65, respectively, compared with unscreened women [29].
The vaccine"s efficacy against HPV type 16 and 18 infection was estimated from available clinical trials [13,32,33], without taking cross-protection against HPV types other than 16 and 18 into account in the base case. The proportion of high-risk HPV was estimated from three studies in Indonesia [34–36]. Although the duration of immunity induced by vaccination is formally unknown, we assumed lifelong vaccine-induced protection in the base case as in other studies [37–39]. We also assumed that vaccination would be performed only at the start of the followed cohort (i.e., at age 12 years), with vaccination decreasing the transition probabilities from susceptible to cervical cancer. Vac- cine coverage was assumed to be 76.6% on the basis of school enrollment rates [40] and the coverage of other vaccinations (measles, diphtheria, and tetanus for 7–12-year-old girls) in Indonesia [41].
Costs and Utilities
In this study, all costs were converted to 2013 international dollars (I$), using purchasing power parities conversion factors [42]. With respect to the economic perspective, we considered only direct medical costs for cervical cancer treatment and all VIA screening–related activities according to the national tariffs for primary and secondary health care services [28]. Cervical cancer treatment costs (both initial and recurrent) were weighted by the cervical cancer treatment patterns for each stage of cervical cancer in Indonesia [34–36,43–46], and applied for every newly detected cervical cancer patient. The total cost for initial and recurrent treatments was I$4140 and I$3169, respectively. In the absence of a national vaccine price and availability of related relevant Indonesian information, we estimated all vaccine- related costs on the basis of Pan American Health Organization (PAHO) revolving fund, which consists of the price of a three-dose vaccination (I$39.71), revolving fund (I$1.39), freight (I$1.19), and insurance and wastage cost (I$1.99) [47]. Thus, our assumption for the total vaccination cost would be I$44.27.
We adopted utilities associated with patients with cervical cancer on the basis of Health and Activity Limitation Index [48], which allows the calculation of quality-adjusted life-years (QALYs) by taking utilities and durations of health states into account. Finally, we systematically applied an annual discount rate of 3% for both future costs and utilities.
Table 1 – Parameters used in the economic model: Base-case values and distributions applied in the probabilistic sensitivity analysis.
| Parameters | Value | Distribution | References |
| Estimated proportion of HPV 16/18 in cervical cancer | 75.40% | Triangular (71.0%; 75.4%; 100.0%) | [34–36] |
| Cervical cancer recurrence | 15.80% | Triangular (3.4%; 15.8%; 23.2%) | [30] |
| HPV vaccination | |||
| Vaccine coverage | 76.60% | Triangular (76.1%; 76.6%; 77.1%) | |
| Vaccine price (I$) | 14.76 | – | |
| Vaccine efficacy-perent reduction in HPV 16/18 persistent infection | 95.00% | Triangular (90.4%; 95.0%; 98.1%) | |
| Screening | |||
| Age range (y) | 30-60 | – | |
| Coverage (3 yearly) | 63.60% | Triangular (50.1%; 63.6%; 70.5%) | |
| Efficacy to cervical cancer incidence | 75.00% | Triangular (59.0%; 75.0%; 95.0%) | |
| Efficacy to cervical cancer mortality | 65.00% | Triangular (47.0%; 65.0%; 89.0%) | |
| Detection rate (confirmed) | 9.90% | Triangular (2.5%; 9.9%; 12.8%) | |
| Cryotherapy coverage | 83.10% | Triangular (13.0%; 83.1%; 100.0%) | |
| Costs | |||
| Initial treatment of cervical cancer (I$) | 4140 | Triangular (2335; 4140; 5825) | |
| Recurrence treatment of cervical cancer (I$) | 3169 | Triangular (1842; 3169; 4415) | |
| Cryotherapy (I$) | 26.29 | – | |
| Screening (I$) | 4.38 | – | |
| Discount rate | 3% | – | |
| Utility | |||
| Susceptible | 1 | – | |
| Cervical cancer | 0.68 | Triangular (0.48; 0.63; 0.84) | |
| Death | 0 | – | |
| Discount rate | 3% | – | |
| HPV, human papillomavirus. | |||
| * Estimated from school enrollment rate and vaccination coverage for measles, diphtheria, and tetanus for 7–12-y-old girls in Indonesia. | |||
| † Includes three doses of vaccine, revolving fund, freight, insurance, and wastage cost. | |||
| ‡ Estimated from the national tariffs and weighted by the pattern of cervical cancer treatment in Indonesia. | |||
Model Outcome
We critically addressed the estimated epidemiologic and economic outcomes from each strategy. Predicted epidemiologic outcomes were the number of both prevented cervical cancer cases and deaths. Furthermore, as an economic outcome, we estimated the incremental cost-effectiveness ratio (ICER) from the incremental costs divided by the incremental QALYs from preventive strategies, compared with no intervention. All out- comes were expressed for a cohort of 100,000 women through their lifetime in Indonesia.
Scenario and Sensitivity Analysis
We investigated the robustness of the ICERs by developing several scenarios with regard to booster dosing at age 30 years (scenario I) if the booster dose would be required to obtain lifelong effectiveness of the vaccine. We also investigated the effect of cross-protection against HPV types 31/33/45/52/58 at 25% efficacy (scenario II: low cross-protection) [33] and at 53% efficacy (scenario III: high cross-protection) [13].Also, we considered limited duration of vaccine-induced protection, specifically at 10 years (scenario IV: short protection) and at 20 years (scenario V: medium protection) and waning of vaccine-induced immunity at 95% efficacy for 10 years, followed by exponential decrease at 50% efficacy during each following period of 20 years (scenario VI: slow waning) or 5 years (scenario VII: fast waning).
We based the vaccine price on PAHO revolving fund for the base-case scenario [47]. In sensitivity analyses, we also explored potential reductions in the market price (75%, 50%, and 25% discounts on I$125.17) [50,51], both with and without booster dosing. Price reductions indicate potential advantages of economic up scaling and tendering effects if widespread vaccination would be considered to be implemented.
Univariate sensitivity analyses were performed by estimating the ICERs on the basis of changes in maximum and minimum values for each parameter and assumption, so as to investigate the most influential parameters or assumptions in the model. Parameters included in the univariate sensitivity analyses were vaccine efficacy, vaccine coverage, efficacy of VIA screening for cervical cancer incidence and mortality, screening coverage, utilities for patients with cervical cancer, and cryotheraphy coverage and its costs.
Probabilistic sensitivity analysis was taken into account by drawing one value for each parameter from its respective distributions simultaneously and estimating the ICER for each strategy correspondingly. We repeated this process up to 1000 times to provide a range for the ICER. We developed a cost- effectiveness acceptability curve to describe the relationship between potential Indonesian cost-effectiveness thresholds and the ICER, using the net monetary benefit approach. Based on the WHO’s criterion [24], a new intervention in Indonesia would be deemed very cost-effective and cost-effective if the ICER would be less than 1 time and 1 to 3 times the gross domestic product (GDP) per capita [52], respectively (2013 GDP per capita was I $3475).
 |
Fig. 2 – Estimated annual cases of cervical cancer prevented (A) and life-years saved (B) by VIA screening, or VIA screening in combination with HPV vaccination. HPV, human papillomavirus; VIA, visual inspection with acetic acid.
|
Results
Clinical Outcomes
The projected annual reduction in cervical cancer cases and deaths as a consequence of VIA screening or in combination with HPV vaccination is presented in Fig. 2. Because the cervical cancer progression increases strongly after the age of 40 years, the effect of cervical screening is most evident in those particular ages. All susceptible women in the VIA screening group have an equal risk again on cervical cancer to that of unscreened women when the screening program stops after the age of 60 years. In contrast, women in the vaccination group remain protected by the effect of HPV vaccination until the end of the model analysis. Assuming a 3-year screening coverage of 63.6% [29], screening would reduce the total incidence of cervical cancer from 1842 cases to 1697 cases (7.9% reduction) compared with no intervention. In addition to the screening, the effectiveness of HPV vaccination in reducing the incidence of cervical cancer is high, as shown in Figure 2A. Specifically, it reduces the incidence of cervical cancer by up to 58.5% and 55.0% compared with no intervention and screening alone, respectively.
The effectiveness of VIA screening and HPV vaccination in reducing mortality would increase gradually after 30 years and attain a peak at 65 years after introduction. Fig. 2B shows that the addition of HPV vaccination on top of cervical cancer screening would prevent substantial mortality. Specifically, these strategies reduce cervical cancer–related death during lifetime by 24.58 and 97.49 cases per 100,000 women for screening alone and screening plus vaccination, respectively.
Costs, QALYs, and ICERs
Discounted costs and QALYs from each strategy are presented in Table 2. Discounted costs and QALYs from VIA screening combined with HPV vaccination (I$5,588,654 and I$2,724,504) are higher than discounted costs and QALYs from VIA screening alone (I$3,393,833 and I$2,723,129), both compared with no intervention. We also estimated that the ICER of VIA screening combined with HPV vaccination (I$1863) would be slightly lower than the ICER of VIA screening alone (I$3126). Apparently, based on PAHO revolving fund policy, both ICERs were still lower than the GDP per capita of Indonesia in 2013 (I$3475).
Table 2 – Discounted costs and QALYs and cost-effectiveness in the base case for VIA screening and vaccination in a cohort of 100,000 women followed from age 12 to 100 y.
| Base case | Cost | QALYs | Incremental | ||
| Cost | QALYs | ICER | |||
| No intervention | 2,486,717 | 2,722,839 | Reference | Reference | Reference |
| VIA screening | 3,393,034 | 2,723,129 | 906,317 | 290 | 3126 |
| VIA screening þ HPV vaccination | 5,588,654 | 2,724,504 | 3,101,937 | 1665 | 1863 |
| HPV, human papillomavirus; ICER, incremental cost-effectiveness ratio; QALY, quality-adjusted life-year; VIA, visual inspection with acetic acid. | |||||
Sensitivity Analysis
The impact of all scenarios on costs and QALYs is presented in Table 3. An addition of a booster dose to achieve lifelong protection has a limited effect on the ICER (I$3040). In addition, vaccine- induced cross-protection against type 31/33/45/52/58 would increase the ICER up to I$1716 and I$1570 for low (scenario II) and high cross-protection (scenario III), respectively. The duration of vaccine-induced protection and waning immunity has a significant effect on the ICER. Specifically, a short duration of vaccine- induced protection (scenario IV) affected the ICER strongly, raising it up to 5 times higher than the ICER in the base case (I$8795).
We also investigated the influence of the vaccine price (com- pared with the assumed market price) for both with and without booster dose scenarios (Fig. 3). The implementation of HPV vaccination on top of VIA screening in Indonesia would not be cost-effective under the normal market price of HPV vaccine (I $125.17) because the ICER would be far above the Indonesian cost-effectiveness threshold of I$10,425 per QALY gained (notably, I $17,106 per QALY without a booster dose and I$27,092 per QALY with a booster dose). If a booster dose is not required to obtain lifelong protection, a 50% reduction in the vaccine’s marketprice (I $62.59) would achieve the ICER (I$8466), being below the threshold. With the booster dose taken into account, a 75% reduction (I$31.29) keeps the ICER (I$6,642) below the threshold [24,52].
We performed a probabilistic sensitivity analysis by running a Monte-Carlo simulation to test the robustness of the model regarding the uncertainty surrounding the input parameters. A cost-effectiveness acceptability curve is presented in Fig. 4. Applying a threshold of 1 time the GDP (I$3475), the probability to be cost-effective would be 72.2% and 99.8% for VIA screening alone and VIA screening combined with HPV vaccination, respectively. In addition, the full range of simulations fell below I$7200/ QALY and I$3150/QALY for VIA screening alone and VIA screening combined with HPV vaccination, respectively.
We tested the influence of each parameter’s changes on the cost-effectiveness ratio in a univariate sensitivity analysis. A minor change in a very sensitive parameter that alters the ICER strongly would be found on the top in the tornado diagram. We see that the most sensitive parameters in the VIA screening strategy are the utilities, the discount rate, and cervical cancer treatment costs. In addition, the ICER was mildly sensitive to cryotherapy coverage, detection rate of screening, cost of recurrence, and VIA coverage (Fig. 5A). The most sensitive parameters in the HPV vaccination in addition to VIA screening strategy were discount rates, utilities, and cervical cancer treatment cost (Fig. 5B).
Discussion
We developed a population-based Markov model to determine the cost-utility of cervical cancer prevention programs in Indonesia, including VIA screening with or without HPV vaccination. Our study revealed that either screening alone or screening in combination with HPV vaccination can relevantly decrease the incidence of cervical cancer and improve quality of life and survival. Because most of the developing countries, including Indonesia, have no explicit cost-effectiveness criteria to justify the implementation of a new intervention, we applied the WHO’s recommendation on cost-effectiveness thresholds, stating that an intervention can be categorized as a cost-effective intervention if the ICER lies below 3 times the GDP per capita [24]. Because the GDP per capita of Indonesia in 2013 was approximately I$3475 [52], both VIA screening (I$3126) and VIA screening in combination with HPV vaccination (I$1863) compared with doing nothing can be considered as very cost-effective strategies. Specifically, the most cost-effective strategy is the combination of VIA screen- ing and HPV vaccination. To our knowledge, this is the first cost- utility analysis of cervical cancer prevention strategies in Indonesia. However, the result of this study, that HPV vaccination on top of cervical screening could be a cost-effective intervention, is in line with results of previous studies in other developing countries [53–58].
Table 3 – Discounted costs and QALYs and cost-effectiveness of various scenarios in a cohort of 100,000 women followed from age 12 to 100 y for vaccination in combination with VIA screening vs. natural progression of cervical cancer.
| Scenario | Cost | QALYs | Incremental | ||
| Cost | QALYs | ICER | |||
| Scenario I: Booster dose | 7,548,979 | 2,724,504 | 5,062,262 | 1665 | 3040 |
| Scenario II: Low cross-protection | 5,506,716 | 2,724,599 | 3,019,999 | 1760 | 1716 |
| Scenario III: High cross-protection | 5,414,894 | 2,724,704 | 2,928,178 | 1865 | 1570 |
| Scenario IV: Short vaccine-induced protection (10 y) | 6,679,563 | 2,723,316 | 4,192,846 | 477 | 8795 |
| Scenario V: Medium vaccine-induced protection (20 y) | 6,603,330 | 2,723,449 | 4,116,613 | 610 | 6754 |
| Scenario VI: Slow waning of immunity (after 10 y, efficacy decrease 50% every 20 y) | 6,391,817 | 2,723,674 | 3,905,100 | 835 | 4678 |
| Scenario VII: Fast waning of immunity (after 10 y, efficacy decrease 50% every 5 y) | 6,630,473 | 2,723,395 | 4,143,756 | 556 | 7458 |
| ICER, incremental cost-effectiveness ratio; QALY, quality-adjusted life-year; VIA, visual inspection with acetic acid. | |||||
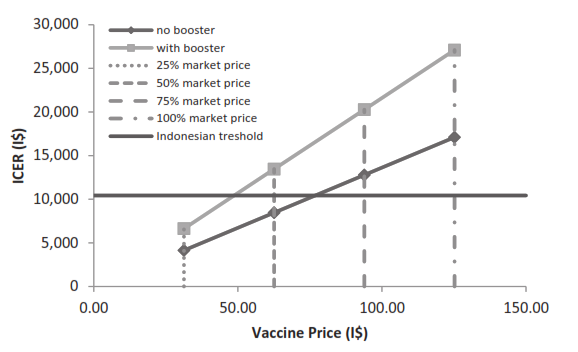 |
| Fig. 3 – The effect of market vaccine price on ICER in terms of booster dose is needed (black square) and not needed (gray square) to achieve lifelong protection. ICER, incremental cost-effectiveness ratio; I$, international dollar. |
Because the long-term efficacy of the current HPV vaccination has not been established, we investigated the possibility that a booster dose would be needed to achieve lifelong protection. As expected, the addition of a booster dose yielded a higher ICER, but the value itself remained below the GDP per capita of Indonesia. This finding is also in accordance with other studies in several settings [37,57,62]. Moreover, the vaccine’s effectiveness is influ- enced not only by the implementation of a booster dose but also by other variables such as vaccination coverage, the distribution of HPV types, and adherence [29,57].
In this study, the effect of cross-protection against HPV types 31/33/45/52/58 is limited, as illustrated by limited reduction from I$1630 in the base case to I$1488 and I$1346 for scenarios with low and high effect of cross-protection, respectively. This finding is similar to that from several studies from other countries that investigated the effect of cross-protection on cost-effectiveness [38,63]. Despite the fact that the distributions of HPV types in various countries are evidently different [34–36] and that this considerably influences the overall vaccine effectiveness from a clinical perspective, cross-protection against other high-risk HPV types can be highly interesting in other settings in Southeast Asia.
 |
| Fig. 4 – Cost-effectiveness acceptability curve, specifically 1 to 3 times the gross domestic product per capita is indicated with the corresponding probability to be cost-effective. HPV, human papillomavirus; I$, international dollar; QALY, quality- adjusted life-year; VIA, visual inspection with acetic acid. |
 |
| Fig. 5 – Univariate sensitivity analyses for VIA screening alone (A) and VIA screening combined with vaccination (B) compared with no intervention. CC, cervical cancer; QALY, quality-adjusted life-year; VIA, visual inspection with acetic acid. |
Based on a vaccine price derived from the PAHO revolving fund policy, the addition of vaccination yielded a cost-effective strategy in preventing cervical cancer. Yet, at the current market price of HPV vaccines, it appears that the addition of HPV vaccination to VIA screening is not a cost-effective intervention in Indonesia. Reduction in the range of 50% to 75% from the vaccine’s market price is required to maintain HPV vaccination in combination with VIA screening as a cost-effective strategy. This result suggests that a reduction in HPV vaccine price, compared with the market price, will be essential for the HPV vaccine to be included in the immunization schedule in Indonesia.
Notwithstanding the lack of data related to cervical intraepithelial neoplasm or precancer in Indonesia, our model can still be considered to validly and adequately estimate the natural history of patients with cervical cancer in Indonesia on the basis of actual epidemiological data from the WHO. For example, the natural history of patients with cervical cancer, cervical cancer incidence, and mortality rates for the population at risk could be described and implemented in the model. Notably, fewer assumptions were required in our model than in a more complex Markov structure or even dynamic model because we did not incorporate any transition to HPV infection or staging on pre- cancer and cancer stages. More complex modeling can be embarked upon if more data become available.
Despite the novelty of this study, it still has several limitations. First, we did not take the vaccine protection for low- risk HPV (type 6 and 11) into account. Although the data related to the effectiveness of both vaccines against other types of HPV are already available [64], the information related to the costs and QALYs caused by low-risk HPV in Indonesia is scarce. Second, incorporation of genital warts as a consequence of HPV types 6 and 11 also will introduce further differences in clinical benefits (i.e., QALYs) between both available vaccines in the market. However, to which extend this will be the case should be further investigated [65]. Therefore, further research should be directed at the clinical burden and costs of genital warts in Indonesia to make a more precise comparison between both vaccines. Another limitation in this study is the potential benefit of HPV vaccines against noncervical HPV-related cancers. Anal, vaginal, vulvar, and oropharingeal cancer, recurrent respiratory papilomatosis, and other precancerous lesions were not taken into account in the current model. The inclusion of these types of HPV-induced diseases will increase the savings and quality-of-life gains of HPV vaccination and consequently improve the cost-effectiveness of HPV vaccination [66–70].
Although we assumed 3-yearly screening in this model, the efficacy of the screening in preventing cervical cancer incidence and mortality is still considerably low. This can potentially be related to the fact that we did not incorporate the cumulative effect of repeated screening in the model [29]. Moreover, women who have negative results on their previous screening noticeably have a lower risk of cervical cancer incidence and mortality than do unscreened women. In this model we assumed that they have equal risk because the straightforward static Markov model has no ability to remember where the patient has come from nor the exact timing of that transition [71]. Yet, univariate sensitivity analysis showed that the influence of screening efficacy on the ICER is very low.
Notably, our results are consistent with results from previous studies from neighboring countries [20–22,38,54,57,58] by con- firming that HPV vaccination in addition to screening can be a cost-effective intervention if it can be obtained at a price similar to, for example, the PAHO price. This finding may encourage policymakers in Indonesia to further consider, decide, and implement optimal cervical cancer prevention strategies.
Conclusions
The addition of HPV vaccination on top of VIA screening in Indonesia, even in the context of various conservative assumptions (need a booster dose to obtain full protection, low cross- protection, short vaccine protection, and fast waning immunity), is a very cost-effective strategy. Substantial clinical and economic benefits can be obtained by implementing an HPV vaccination program. Nevertheless, improvement of the screening program itself also remains important and provides further potential to achieve optimal cervical cancer prevention strategies.
Acknowledgment
We thank Dr. Agusdini Banun Septaningsih from “Dharmais” National Cancer Hospital, Indonesia, for her advice on unit cost estimates in Indonesia.
Source of financial support: This work was supported by the Directorate General of Higher Education (DIKTI) Scholarship, Ministry of National Education, Indonesia. The authors’ work was independent of the funders, who had no role in the study design, analysis of data, writing of the manuscript, or the decision to submit for publication.



Tidak ada komentar:
Posting Komentar